
The AED operator is responsible for ensuring that the correct defibrillation process is followed; however, a more qualified and/or experienced lifesaver (such as an ART holder) will be team leading the resuscitation and coordinating the other lifesavers involved.
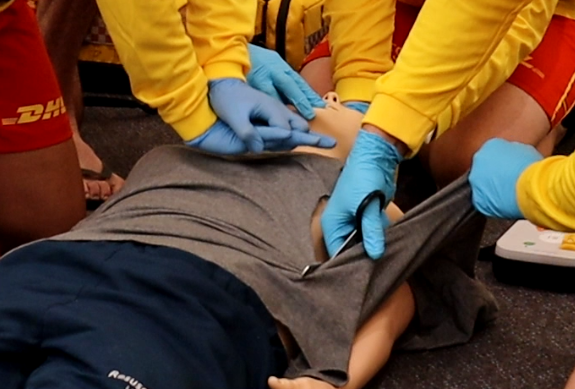
As per team CPR roles described earlier in this chapter, CPR should be commenced and continued with minimal interruption until the AED is ready to analyse. In team CPR, Operator 3 approaches the scene to the patient’s left, placing the AED in the 2 o’clock position. Operator 3 is to remove clothing, working around the operator performing compressions, without interrupting CPR. Trauma shears are recommended to cut through clothing, underwear and wetsuits, ideally down the side of the body. Practicing cutting clothing with trauma shears during training is strongly recommended.

The AED / airway operator (Operator 2) will be responsible for analysing and shocking the patient if required. They should follow the AED operator’s instructions leading up to the AED analysis and advise to shock or not shock the patient.
- Always check that conditions are safe for the use of an AED
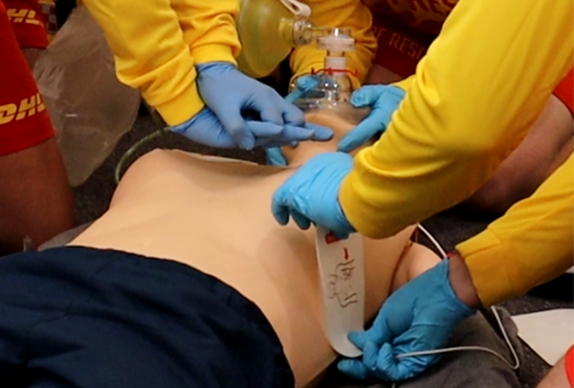
- Operator 3 cuts clothing, then turns on AED, and prepares / applies AED pads
- After applying the AED pads and turning the AED on, Operator 3 informs Operator 2 that the AED is turned on, and pads have been applied. They then prepare to take over compressions, with their hands hovering over the patient’s chest, awaiting instruction of Operator 2
- Following the AED prompts, Operator 2 verbalises “stand clear”, while hovering one hand over Operator 3’s hands and the other prepared to push the shock button, if advised to do so by the AED. Ensure no one is touching the patient prior to delivering shock. Deliver a shock in a safe manner if prompted, followed by tapping the compression operator’s hands and announcing “shock delivered, CPR-Go”
- Re-start compressions upon these physical and verbal instructions from Operator 2
- After 2 minutes of CPR, the AED will recommend analysis again. Operator 2 to follow step 4 again. Operators 1 and 3 swap roles.
AED prompts lag behind the physical shock delivery, which can lead to delays restarting compressions. This reduces the overall chest compression fraction, which we are aiming for a target of 80%. There is no danger to rescuers re-starting CPR within seconds of shock delivery, and with practice in the team environment, the delays to restarting compressions can be minimised.
As previously mentioned, signs of life take time to appear, and CPR should be continued until signs of life become obvious. Operator 2 returns to the jaw thrust position, and if oxygen is in use via the bag-valve mask, reattaches this with the resuscitation mask once compressions are re-started by Operator 1 or 3, with the BVM squeezed by whichever Operator is not undertaking compressions.