
Anaphylaxis is a severe allergic reaction that requires immediate management with an adrenaline auto-injector prior to calling an ambulance. It is potentially life threatening as a common symptom is upper airway obstruction, hypotension or bronchospasm.
Anaphylaxis usually occurs within 20 minutes to 2 hours of exposure to an allergen to which a person is already extremely sensitive. You should always treat it as a medical emergency.
Signs and symptoms
- Abdominal pain and vomiting
- Becoming pale and floppy (in young children)
- Difficult/noisy breathing or persistent cough
- Difficulty talking
- Dizziness, loss of consciousness or collapse
- Hives, welts and body redness
- Itchy or running nose
- Swelling of face, eyes, lips and tongue
- Swelling/tightness in throat
- Watery eyes
Management
- Remove any exposure to potential allergens.
- Lay the person flat or allow them to sit still if breathing is difficult lying down.
- Administer an adrenaline auto-injector into the person’s outer mid-thigh as per the instructions label on the device.
- Hold the device in place for the time stated on the instructions label of the device.
- Send for help, additional resources (another adrenaline auto-injector, asthma medication if possible and an AED) and request an ambulance.
- Monitor and reassure the person while waiting for paramedics to arrive.
- Administer a second adrenaline auto-injector if there is no response/improvement of the person after 5 minutes and if one is available.



✓ DO
- Ask them if they have an individual anaphylaxis action plan.
- Follow the instructions of the ambulance service.
- Always administer an adrenaline auto-injector as per the manufacturer’s instructions.
- If possible, assist the person to administer their own adrenaline auto-injector before sending for help.
- Commence CPR and apply an AED if the person becomes unconscious and is not breathing normally.
✖ DO NOT
- Use an adrenaline auto-injector on infants under 7.5kg unless indicated on their individual anaphylaxis action plan.
- Rub the injection site.
Note
- When administering a second adrenaline auto-injector (if required), administer to the person’s other outer mid-thigh if possible. This will help reduce any pain at the first injection site.
- If the person has asthma and is also at risk of anaphylaxis, the adrenaline auto-injector should be used first, followed by the asthma reliever medication.
- If an adrenaline auto-injector is not available for an anaphylactic person, give asthma reliever medication if the person is conscious.
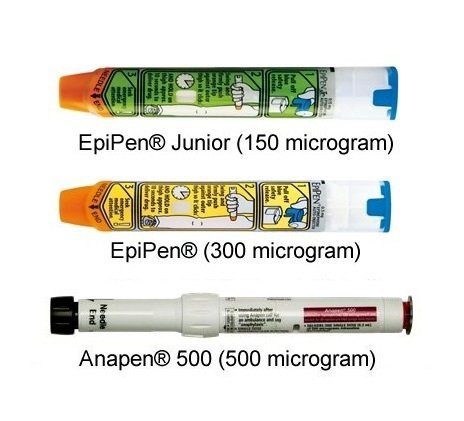
- An adrenaline auto-injector containing 300 micrograms can be used on a young child (7.5 – 20kg) if an injector with a lower dose is not available.
- An adrenaline auto-injector containing 500 micrograms can be used on a child over 20kg if an injector with a lower dose is not available.
- Expired adrenaline auto-injectors or ones with discoloured adrenaline are not as effective when used for treating anaphylaxis. However, they should be used in preference to not using one at all. Advise the person of any potential issue with an adrenaline auto-injector and gain their consent to use it.
- First responders qualified in advanced resuscitation may safely administer oxygen to persons showing the signs and symptoms of anaphylaxis. Refer to the SLS Pathways website or the appropriate person at your SLS club for more information on advanced resuscitation training.
- Adrenaline auto-injectors contain a synthetic version of adrenaline – epinephrine. Further information regarding these auto-injectors can be accessed via the ASCIA (Australian Society of Clinical Immunology and Allergy) webpage and Allergy & Anaphylaxis Australia (A&AA).
- Refer to the latest ARC Guideline for the management of Anaphylaxis or allergyfacts.org.au to learn more.