
High quality compressions are key to a successful resuscitation.
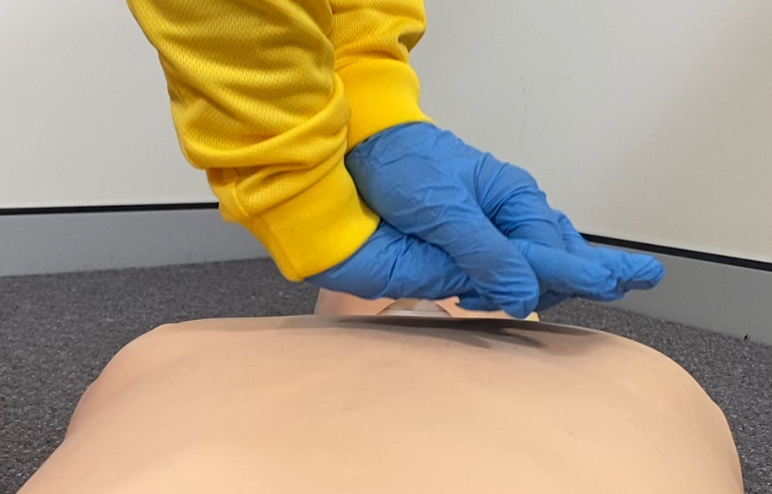
Hand positions
The methods described here are widely used. Your choice of hand position will depend on the size of the patient as well as your own body size, strength, personal preference and comfort.
Place the heel of your preferred hand over the lower half of the sternum. The exact positioning of your fingers does not matter, as long as the heel of one hand is compressing through the lower half of the sternum. Apply vertical pressure from the shoulders through the heel of the compressing hand. Keep your arms straight, where possible, to use your body weight to apply pressure vertically with your hips acting as a hinge or pivot point.


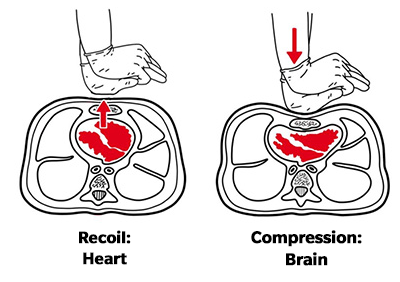
Chest recoil
Hands-off CPR technique involves lifting hands slightly off the chest following each compression. This has been shown to be the most effective method to achieve complete recoil, while allowing adjustment of hand position throughout the compression cycle.
Complete chest recoil allows filling of the heart and its blood vessels, allowing greater chance of a successful AED shock.
A memory aide is “Heart – Brain – Heart – Brain” as you: recoil – compress – recoil – compress.
Chest compression fraction (CCF)
Chest compression fraction refers to the percentage of time during CPR that compressions are being undertaken. A target of 80% allows 20% of time for delivery of rescue breaths and AED analysis/shock delivery protocols within team CPR. Survival in shockable cardiac arrest patients has been shown to improve by over 10% for every 10% increase in compression fraction up to 80%.
Effective compressions improve both blood pressure and energy (adenosine triphosphate, ATP) in the heart muscle cells, and for every second that compressions are paused, these begin to drop. Minimising pauses maintains the blood pressure and energy, meaning an AED shock is more likely to work, successfully converting electrical energy into muscle contraction.
Note: training defibrillators often have a lag in time from analysing to advising shock – the 80% target is for real-life resuscitation.
CCF can be maximised by reducing the frequency and length of interruptions to compressions by a choreographed team approach:
- Breath delivery – count 1 second per breath (x2) then re-start compressions whether or not breaths have been successfully delivered
- AED pad placement – apply pads working around compression operator continuing CPR
- AED shock delivery:
- Swap roles at least every 2 minutes or during AED analysis time
- Hover hands ready to re-start CPR, with a physical and verbal cue “CPR-Go” by the AED operator, without waiting for the AED instructions.