When two lifesavers arrive at a scene where a victim requires CPR, one lifesaver should commence DRSABCD while the second lifesaver calls for assistance and obtains additional equipment and personnel as required, e.g., defibrillator, first responder with oxygen.
If two lifesavers are available to perform CPR, one lifesaver may perform rescue breathing while the other provides compressions. It is recommended that the operators switch providing compressions at least every five cycles (30:2), to prevent rescuer fatigue and deterioration in the quality of chest compressions. This should be done with minimal interruption to compressions.
Compressions may be counted out loud so that others can follow the CPR cycle. At a minimum, it is recommended that the last five compressions be counted aloud.
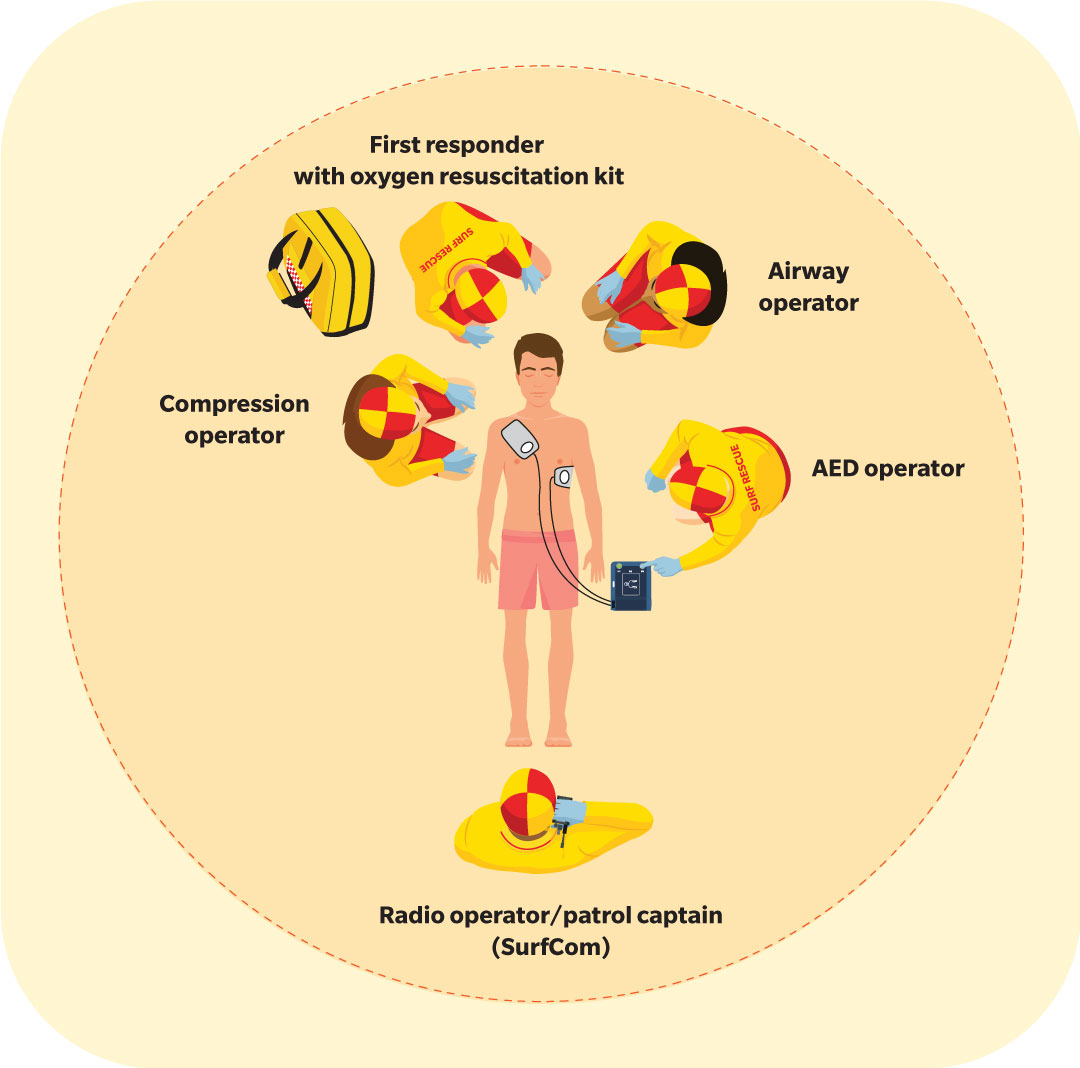
The airway operator who is managing the victim’s airway coordinates the rollovers when a victim regurgitates or vomits. They may be behind the victim’s head if they are using jaw-thrust method to maintain the victim’s airway.
Qualified lifesavers may safely administer oxygen to any victim who is not adequately perfused. Trained lifesavers may assist them with the administration of oxygen-aided resuscitation and oxygen therapy during team CPR. Usually this assistance takes the form of ensuring the appropriate oxygen mask is securely placed over the victim’s airway and keeping the oxygen at a safe distance from potential sources of combustion, e.g., flames, cigarettes, defibrillator.
When additional lifesavers are available to help, they may approach the CPR scene from the victim’s feet to introduce themselves and confirm an ambulance has been called before proceeding as directed by the airway operator.